Happy summer my friends. In Colorado we are starting off with a cool, wet one which is great for the a/c bill but less ideal for exploring outside.
Lot’s going on here including medically.
I had some work travel last month and towards the end I started not feeling well, including being light headed. I mentioned this to my oncology nurse 2 days ago during my treatment appointments and she scheduled a brain MRI and echocardiogram. Yes, light headedness triggers the immediate thought of brain metastasis.
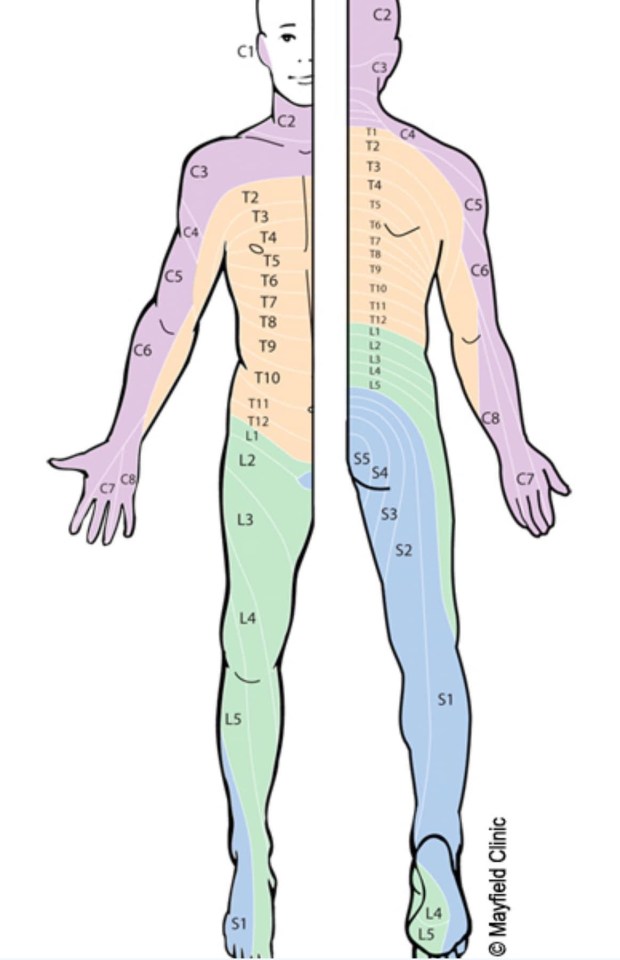
Recall from my last post that we’ve found the MRI to be the best imaging for me. The brain MRI captures the head and top part of the spine (cervical). Mixed results: no brain metastasis 🙌 but it did pick up a new lesion on my C1 vertebrae 👎.
The nerves that come out of the C1 impact the sides of your face and head as shown in this nifty diagram (one of my fav diagrams BTW).
The most likely explanation for my light headedness is that the lesion (tumor) is pressing on the nerves. So, my oncologist has ordered another PET/CT to check again. It seems a little insane to keep getting imaging that doesn’t work so well – I guess he wants to confirm or look for other lesions.
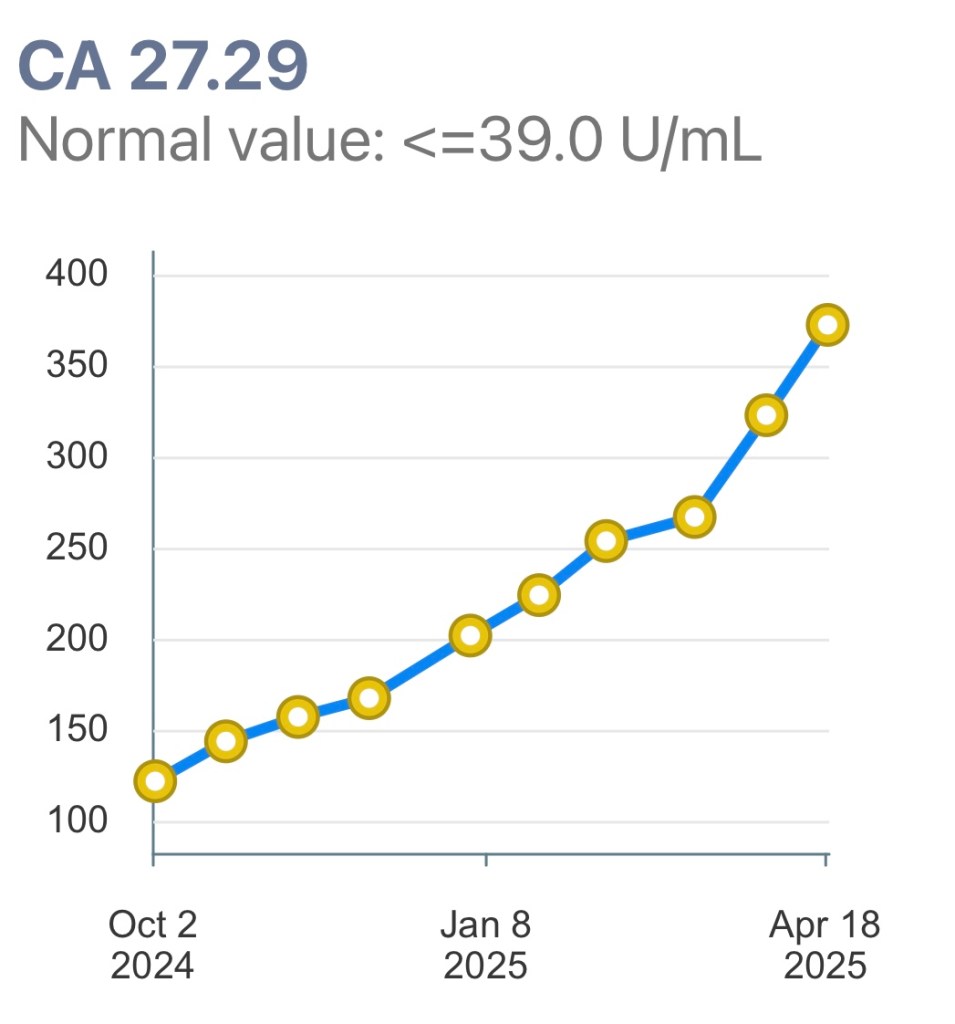
My tumor markers did drop the end of last month which is in contradiction to the new tumor.
See how complicated and tricky cancer is?
For now, I’ll get the PET/CT and an echocardiogram and keep doing all the things (eating healthy, moving, relaxing) and we shall see where this takes me.
After my work trip I spent 2 days in Chicago at the American Society for Clinical Oncology (ASCO) where I learned about new treatment lines coming out and connecting with other patient advocates.
The cancer research going on now will result in the drugs being used in the coming years. This is why it is so important to preserve funding for the National Institutes of Health. The presidents budget slashes funding by almost 50%. That means many fewer clinical trials and many fewer drugs in 5 years. No one expects to get cancer. If you get cancer in 5 years you will be wishing the NIH had done more research to help you. Please call your elected federal reps and push for restoring funding to NIH.
On a lighter note – Maddy graduated from high school, Evelyn started a research internship at University Colorado Anschutz Medical Campus and we all head to Las Vegas at the end of the month to support Maddy in her last National Dance Competition.
Onward!
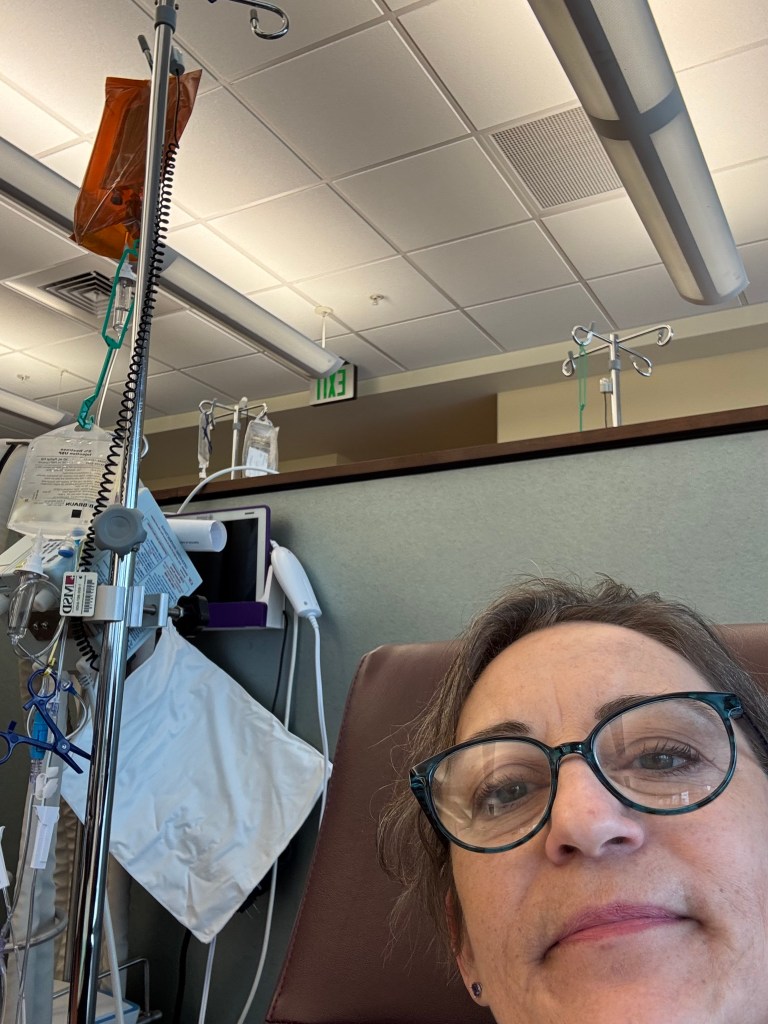
Amir humored me with a selfie in front of the MRI machineMaddy’s pre-professional companyThe ASCO meeting was huge with 50,000 attendeesGrateful Nancy could come for the graduationMy 2 favorite future engineers.
Hi everyone. I write this at the end of a long – but good – day. My legs are up in my recliner and the cat is curled up. I guess he had a long day too.
Today was “treatment day.” That means a lab draw, office visit and then infusion of medications.
I had prepared for today and the real possibility of having to change my treatment. As I always say – I want to stay on each line as long as possible because there are a finite number of options.
Short version – I’m staying on my current treatment, Enhertu. I have a very good quality of life with it. It seems to be working, mostly, we think, maybe.
I get this drug every three weeks so I’m estimating that this means I’ll probably stay on Enhertu through a good portion of the summer.
If you are trying to kill time keep reading. Otherwise get outside and grab some sunshine and fresh air! ☀️
Longer version – I’ve been getting PET scans every 3 months for a little over a year. Previous to that I was getting a CT scan with contrast + nuclear bone scan. Recall I had terrible progression and they had to rebuild my upper thoracic spine in November 2023. The CT + bone scans Did. Not. Show. The. Tumors pressing on my spine!
How is this possible? Imaging is a very imperfect science and a lot of it is a matter of interpretation. And why would I get that particular combination of scans? Money. It’s the cheapest option and that is what insurance will pay for, unless something goes terribly wrong.
Queue fall of 2023. We clearly needed better imaging. The insurance company approved a PET-CT scan. PET scans provide essentially the same info as the CT + bone, but honestly they are better. Oncologists prefer them, insurance companies don’t. The PET-CT scan in December 2024 showed more uptake of the tracer in my thoracic spine. Diseased cells take up more of the tracer. These hot spots – or spots of increased uptake could mean the cancer is active and growing (progressing).
I had another PET-CT in March 2025 and it showed even a little more increased uptake in those areas – which made it seem like I was having progression, especially because my (very reliable) blood work tumor markers were steadily rising.
Now, I’ve been at this for a while – almost 6 years actually. I understand what is going on and I know what to ask for. I know that imaging doesn’t really work well for my cancer, unless it’s an MRI. I requested we do an MRI of my thoracic spine to see exactly what was going on. An MRI produces a very detailed image of every part of the internal structure of what is being scanned. My oncologist agreed and I had an MRI last week (on Sunday afternoon no less).
The results of the MRI were – unremarkable! (Love that word!) No tumors growing in my spine. Nothing of note in my thoracic spine. My lumbar spine has some bulging (L1, L2) and severe compression deformities (L3, L4) – which we already knew.
[Side bar – I have lobular breast cancer which typically doesn’t show up well on imaging because it doesn’t clump or form in a lump usually. Also, when it metastasizes it goes to unusual places like the stomach, colon, bowel, bladder and peritoneum and forms in thin sheets or strings, neither of which show up on imaging.]
Image from the Lobular Breast Cancer Alliance showing where mILC can metastasize.
Fast forward to today. My oncologist is totally comfortable with my staying on Enhertu given that the MRI didn’t show anything of concern. My CA 27-29 tumor marker is steadily rising. Historically my tumor marker has been reliable in indicating progression (rising numbers).
Tumor markers give an indication of how active the cancer is. A number below 39 means no active cancer. I’ve never had my tumor marker go below 42 the entire time I’ve had metastatic breast cancer.
My oncologist considers three things when recommending changing medication:
Imaging results
How the patient feels
Tumor markers numbers
Clearly imaging does not do a great job at indicating progression and the MRI didn’t indicate anything alarming. I feel great (working FT, walking an hour a day, just signed up for Pilates 2x a week). My tumor markers suck.
So, stay the course it is. Is this the right decision? 🤷♀️ We think so.
Before I had metastatic cancer, I didn’t appreciate how complicated making decisions was. I’ve learned that science has miles to go improving imaging so that it is more reliable. New in the past few years is the use of measuring circulating tumor cells in the blood, so that may eventually be a tool in the future for oncologists to figure out what is going on and base decisions on.
I appreciate my relationship with my oncologist. Everything is a joint decision. He listens to me (said yes to my suggestion of the MRI). He keeps current on the science and research. We are looking into a possible clinical trial for when it is time to switch medications. I’m grateful that I have access to such good medical care (and currently have very good insurance that allows me such access).
So, my health world right now is good (as are things with the girls). A lot of other parts of life are challenging and stressful. I’ll continue to take things one day at a time and live life to the fullest. I hope you do too. It passes quickly and this is our only chance to seize the day!
Onward!
Today I had a window seat for my infusion. The foothill mountains are green and you can still see snow on the Continental Divide. How wonderful that I have this view.The brown bag has my Enhertu. Once it’s mixed up it can’t be in direct light. I also get fluids (the big bag) and before this I had pre-meds including steroids and 2 kinds of anti-nausea meds. All total I spend ~3 hours at the Cancer Center.
Hello friends and family! A quick update on things cancer-related, as you can expect from this blog!
My hip is fantastic. No pain at all. I’m up to walking around 4 miles a day. I can manage about an hour at a time. So happy about that and grateful for the skill of my orthopedic oncologist Dr. Lerman.
This coming Monday morning I will have treatment #21 of Enhertu. Recall this is a drug called an Anti-body Drug Conjugate (ADC) and is given intravenously every three weeks. Overall this drug has been good to me. It brought me back from the brink of a run-away cancer train early last year. Recently it’s not clear it’s been working so well as I mentioned in this post. Recall also that this drug was approved for my type of breast cancer (Her2-low) only in August 2022 – a full 3 years after I was diagnosed with MBC. I’m hoping for more drug discovery and approval so I can live longer!
I’m grateful that my side effects continue to be minimal. I’m on a blood thinner because it caused a blood clot last fall. I take Olanzapine nightly to control nausea and vomiting. I’m also grateful for the researchers that looked into this particular use of Enhertu. So very grateful!
This brings me to my second update. The future of cancer research in the U.S. is at risk. I know this first hand as a researcher I work with is looking at a loss of funding from NIH for his basic lobular breast cancer research. He shared some of the graphics and information shown here.
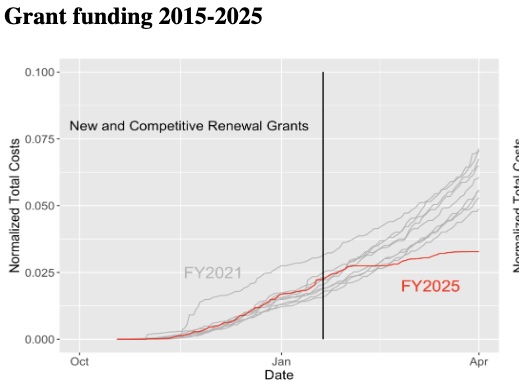
This chart shows the trends of NIH grant funding from 2015-2025 (source). As you can see, the amount of funding being distributed is far below previous years. The spring months (Feb-May) is when most federal awards are made based on the budget cycle.
Screenshot
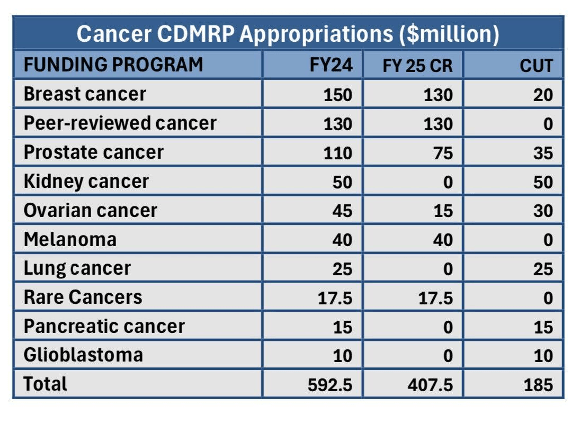
The outlook for the Congressionally Directed Medical Research Programs (CDMRP) show significant cuts to cancer research. The March 14 Continuing Resolution has their budget reduced by 57%. You can see from this chart where some of the cuts were.
You may say, well ok, but there are a lot of other sources of funding for cancer research. There are other countries who will continue research – we don’t need to worry. Not really. As you can see from this chart, the NIH is BY FAR the largest funder of cancer research IN.THE.WORLD! The budget of the NIH is significantly larger than the next largest funder.
Ok, you say – what about foundations? They also support research. Yes, they do. The amount that they spend is a fraction of what the U.S. Federal government spends. In addition, the dollar amounts from foundations tend to be small. The motivation of foundations is to provide seed money to develop a proof of concept. Once the researcher does this they have some preliminary data to seek out a federal research grant to do the main research. The foundations take on the risk that federal funding won’t.
Well, Donna, thanks for giving me such uplifting news. Now I feel sad. Well, I can help you feel better about all of this by – please – contacting your federal elected representatives and urge them to restore funding to the NIH. You can find their contact info here. If you scroll down past the photos you can see a script to follow when you call.
All this being said, I remain cautiously optimistic that Americans will band together and convince our reps to fund cancer research. You never know who will get cancer next and having new treatment options is critical.
Onward!
I encountered this lovely little duck swimming away in the creek on my walk in Lafayette.Grateful my neighborhood has some nice views for my short walks.
Script for federal reps:
Hi, my name is [Name] and I’m a constituent from [Your city].
I’m calling to urge [Name of representative] to oppose the recent devastating cuts to NIH funding and staffing. These cuts are already disrupting crucial research to treat diseases such as cancer [you could also add Alzheimers, diabetes, other diseases that impact you]. Hurting the NIH hurts everyone.
Thank you for your time and consideration.
p.s. If you leave a voicemail be sure to leave your full street address to ensure your call is counted.
p.p.s. – If you are nervous about talking to a person, call in the evening and leave a voice mail. It still counts.
Hi friends and family – I hope spring has sprung in your area and you’ve been able to enjoy some time outside!
I write to share the latest status of my life with MBC and treatment. On March 31 I had treatment #20 of Enhertu! Yippee! Enhertu is an anti-body drug conjugate (ADC) given intravenously every three weeks. I do not have a port for it. On days I receive treatment I’m at the cancer center anywhere from 3-5 hours.
My oncologist considers three things when determining if we stay on the current treatment or change.
How do I feel?
What does imaging show?
What are my tumor markers (blood work) showing?
Fortunately, I feel quite good. I am still working FT. I’m walking daily. I’m doing all the things I want to do. So, all good here.
Imaging. Earlier in March I had a PET scan to see if the cancer is active. The imaging report stated that there was increased activity in several areas of my spine. My scan in December also showed a small increase in activity. So, not the best result.
Tumor Markers. My tumor markers (CA 27-29) have been steadily rising, not great. Ideally we want the number to be under 40. As you can see from the chart here, they are above that and trending upward.
Screenshot
So, what to do? 2 out of the 3 indicators are pointing to progression. My oncologist gave me the option to change medication now or stay on Enhertu. He said it is the “devil you know vs. the devil you don’t know.” After some discussion we agreed that if my tumor marker got into the 350-range we’d change meds.
Keep in mind that when we had that conversation I didn’t have my most recent tumor marker number. Clearly, it has jumped a lot in the past 3 weeks.
So, what next?
As long as I’m still feeling fine I will have my next appointments and treatment on April 12. However, it remains to be seen if I’ll have Enhertu or the next medication we have lined up (also IV chemo).
As you know, there are limited treatment options so we aim to stay on them as long as possible. On the other hand, we don’t want to stay on a treatment that is not working. We want to find something new that will quiet the cancer.
I leave you with a few photos from some recent travels. More soon.
Onward!
At the pool (Hearst Castle, CA)The crew whale watching (CA)Enhertu treatment. Enhertu has to be mixed on site and then covered with a brown bag to block sunlight.
Wow, I realized it’s been a hot minute (actually 2 months) since I shared an update on my health. You can assume that no news is good news!
I’ve been busy life-ing. I’ve been focused on improving my movement. I haven’t used a cane since October. I’m up to walking an hour at a time up to 3mph. I have started some weight training at home, basically trying to get back into shape.
All this to say, I’m feeling fine. I still have continual pain medication and other meds to deal with side effects. Other than some fatigue I’ve been feeling pretty good.
I’m still getting IV chemo (Enhertu) every three weeks. I’ve been on this medication since February 1 of last year. I’ve been grateful to have tolerated it so well.
There are hints though that it might not be working so well any longer. My scans in December were “fuzzy” and I just had another PET scan this morning so I will learn soon if the cancer is quiet or progressing. My bloodwork tumor markers have been rising pretty steadily (bad) so that is a concern.
I next see my oncologist at the end of this month and we will determine then if I need to change meds or not. As you all know, it’s best to change the medication if it is not keeping the cancer quiet. There are a finite number of medications though so the goal is to stay on each one as long as possible.
Our family is headed out on a little holiday later this week to celebrate life. Life is short! Go do “all the things” – even if it doesn’t seem like the best timing.
Onward!
Cheering on the BroncosEvelyn and Glen skiingMaddy and Grandma SeifertI dropped something off at Ev’s apartment and we snapped a quick selfieWith my MBC Sisters. I went to a conference with 350+ women living with MBC. Such love!
It’s been an interesting week, regardless of who you are and what you support. I’m writing because one of the Executive Orders this week puts a freeze on communications from many Federal agencies including Health and Human Services (HHS) and the National Institute of Health (NIH).
This is a serious situation as it is already putting cancer research at risk. I work closely with a breast cancer researcher at the University of Colorado (Dr. Matt Sikora) who conducts basic research through grants from NIH. Based on communications he received, it looks like his research lab may lose funding. This funding supports the basic cancer research that leads to new treatments. We all know how I feel about new treatments!
Well, that is a lot. What can I do as one individual?
I ask that you take 10-15 minutes to send an email to your elected members of Congress (you have 2 state Senators and 1 Representative). Believe it or not, staffers count the number of communications they get from constituents on a particular topic. While you might get a form letter response, don’t get discouraged. They will count your email! It will make a difference.
To help you, Dr. Sikora has drafted a sample email and provided links to find contact info for your elected reps as well as a link to where you can find the economic impact of cancer research in your state.
I’m happy to help anyone if you need it. Thanks for your consideration. Cancer has long been a non-partisan issue and should stay that way.
Onward!
Sample email text (you need to change things in bold)
Dear [congressperson]:
I am writing due to grave concerns with the freezing of communications at Federal agencies. Specifically, I am writing regarding HHS and the National Institutes of Health, including the indefinite suspension of council review meetings, review study sections, and travel. Suspension of these meetings and review sections jeopardizes biomedical research funding nationwide.
Currently, our state of Colorado receives nearly $600 million in funding for biomedical research from NIH, supporting over 7,000 highly skilled jobs and driving over $1.5 billion in economic activity. As a concerned constituent living in [Denver], and as a [patient living with cancer/research advocate/caregiver/etc], I urge you to make sure that money that has been allocated for NIH extramural funding, including all training and workforce development grants, remains committed. Loss of this funding would be disastrous for our local economy, and would drive major job loss including in highly trained university biomedical research personnel, including graduate students and postdoctoral trainees that make up the next generation of biomedical researchers.
NIH has always benefitted from robust bipartisan support, and I urge you to continue to commit Federal support to the NIH mission and extramural program, which ensures that our nation remains at the forefront of biomedical research innovations and advances in patient care.
As New Year’s Day winds down I write to say hello to all my friends and family, near and far. 2024 was actually a pretty good year for me (unlike 2023) and I’m optimistic this year will be even better.
I had a PET scan in December and the results were “fuzzy.” Well, that is the first word my oncologist used. Let me explain.
He agreed that imaging was not very reliable for me. However, the results showed additional uptake of the contrast in a few areas where I have known cancer (mainly in my spine). On the one hand, other areas seemed quiet and unremarkable. (I want to get a t-shirt that says “I’m unremarkable” – if you know, you know.)
Dr. Andorsky said the most important thing is how I’m feeling. I feel great! Really, I am so grateful for my new hip and my fentanyl patch and other meds, and the fact that I can get up every day and work, exercise, read, paint – you name it. On the other hand, my tumor markers have been slowly rising. They tend to be accurate in terms of whether cancer is active or not.
The other thing to consider is that there are a finite number of treatments so you want to make them last as long as possible. I was prepared to argue to stay on the same treatment and I didn’t need to do that at all! He suggested we stay on Enhertu and revisit in 3 months.
In other news, the tingling in my left arm has gone away. I will attribute it to the blood clot I had under my left collarbone and that by this time it has dissolved and so has my arm tingling.
So, I stay the course which is the best possible outcome. I get an IV infusion of Enhertu every 3 weeks. The cancer center is only 5 miles from my house so I’m able to get there and back quickly. A typical appointment is 3-4 hours for labs, an office visit and then treatment.
The rest of life is going swimmingly. We had a lovely (short) visit with family in Wisconsin. Glen, Maddy and Evelyn have hit the slopes already. Evelyn has been popping home now and again. Maddy has a short break from dance so she is home a bit more as well.
Maddy and I head to Texas to see her grandparents, it will be a short visit – we are looking forward to it regardless. I’ve booked a trip to see my BFF in LA for February and our family is making plans for a few family vacations in 2025.
I hope you are able to approach 2025 with optimism, enthusiasm and peace. I hope to see many of you this year. You are always welcome here – we have plenty of room! Seriously, we’d love to show you around Colorado.
Onward!
Annual Nutcracker BalletToulouse loved present debris!Selfie with Mom and AnnYou can’t visit Wisconsin in winter without bowling.
We are in the throes of fall and the Thanksgiving holiday is less than a week away. For many people, this time of year causes more reflection. For me, it’s mostly gratitude.
I’m grateful that I am able to celebrate another holiday season with my family. I’m grateful that most days I can live my life like I don’t actually have a terminal disease. I’m grateful for friends and family that support me and I’m grateful for science and scientific researchers who are working to find more treatment options for me.
I’m grateful that my oncologist is top of the game and is always a step a head of me. I appreciate that because, as you can imagine, I’m the kind of patient that comes with questions about new drugs and clinical trials.
Speaking of which, I spent all of yesterday afternoon researching clinical trials. Clinical trials.gov is a database of every clinical trial happening in the U.S. As you can imagine there are tens of thousands. Fortunately they have a decent search feature.
Even better are two trial search sites that focus on breast cancer. The Storm Riders site allows you to search for any trial related to breast cancer (any stage). It’s a fantastic resource. If you know anyone with breast cancer I hope you will share it with them.
The other site is Metastatic Trial Talk. This one is focused on stage IV, metastatic disease. In spite of searching and reading through many, many trials, I did not find any that were particularly helpful for the next treatment line. That was a little disappointing.
Last month my oncologist shared a trial with me for my next line that basically compares two different types of IV chemo. While that is fine, I’m really hoping for something that doesn’t require me to go in to the cancer center every week for an IV infusion.
I’m still taking Enhertu and the side effects have stepped up their game lately. Actually, I don’t know if they are side effects or just bad luck with something else.
I have tingling in my left arm that comes and goes. I had a Brain MRI and MRI of my cervical spine. The brain MRI was clear (yay!) and the cervical spine showed that the openings in some of my vertebrae where nerves exit are a bit too small and pinching the nerves, potentially causing the tingling.
What is causing this in my cervical vertebrae? I met with my neurologist and they are convinced that it is not a result of cancer. My oncologist thinks the same thing. What did they say? “This kind of thing can happen when you are 50+.” I don’t buy it. I think there is something going on that is causing it, likely cancer.
I also have a blood clot under my left collar bone. That could be causing the tingling. I’m on blood thinners now to prevent any new clots from popping up.
To top things off I’ve been having episodes of vertigo. My PT did the Epley maneuver and that helped initially. However, the episodes continue.
So, where does this leave me? Good question.
I will have an infusion of Enhertu on December 4. I will have a PET scan the following week followed by a telehealth appointment with my oncologist. My CA 27-29 tumor markers have been rising, so that’s not great. At that appointment we will know if the cancer is quiet or progressing. If it’s quiet, we continue on with Enhertu. If it’s progressing, we change treatment.
In between my Enhertu infusion and scan I will need to travel for work. I don’t mind traveling for work but it’s certainly not fun. It’s harder for me now than before my diagnosis so I try to go only when I really have to.
That’s my cancerland part of life. In the rest of life, I’m still working FT. I’m almost finished with a painting project, I’ve started painting with watercolor, and Glen and I went to the theater to see A Christmas Carol. The girls are off in Vienna now, exploring and having some quality sister time.
I hope that all of you have a meaningful Thanksgiving holiday, whatever that looks like for you.
Onward!
Glen and I at A Christmas CarolMy buddy resting with meMaddy turned 18 mid-November
It’s been a busy couple of weeks. The main thing to share is that I feel great and have largely been able to do all the things I’d like to. My main medication (Enhertu) does cause significant nausea and vomiting (yes, that is the reality of MBC) but I have some medication that largely keeps it at bay.
My recovery from the hip replacement is going very well. All restrictions are lifted and I’m working with my PT to get more flexible as well as gain strength and endurance while walking.
October is Breast Cancer Action (Awareness) Month. This year hit differently for me and I can’t pinpoint it. It’s been hard. I did update the blog pages to include my favorite organizations for supporting breast cancer. You can see it here: Organizations to Support. If you are inclined to share some of your hard earned money to breast cancer research you are welcome to donate to my efforts to support METAvivor on this page.
Last month Maddy and I went to Belgium to attend the International Lobular Breast Cancer Symposium. In addition to enjoying the city of Leuven, I learned a lot about the state of research of lobular breast cancer. I have a short write up of what I learned at the end of this post.
Going back to the month of October and breast cancer – please “Think before you Pink” and know where your money is going. Awareness will not help those of us being treated for cancer. Ask questions, if they can’t tell you where the money is going it’s probably not a good investment.
I have treatment again this coming Wednesday. I’m usually at the cancer center for ~4 hours total including office visits, labs and treatment. I use the time to keep up with work but also read – or nap!
Take care of yourselves and your loved ones and enjoy fall.
Onward!
The Town Hall for the city of LeuvenThe river through LeuvenUniversity campus buildingShopping after lunchYou can’t go to Belgium and not have waffles (dessert)Bicycles everywhere!The Symposium was held on campus in a converted church
Here is the summary of my experience at the Symposium:
The ILC Symposium, held in Leuven Belgium, was attended by clinicians, researchers, and patient advocates. I attended the 3-day event as a patient advocate. There were just under 190 people in attendance. There are three main points I took away from the Symposium. Imaging for ILC is not very good and needs a lot of improvement. There are new opportunities for understanding an individual patient’s ILC/disease using circulating tumor cell technology. There are many people passionate about ILC and working to move the needle both in treatment and awareness. I found the opportunity to network with other patient advocates to be very good on Monday. We traveled to the university hospital and the time together on the bus allowed for very informal conversations. On the way back from the hospital we discussed what we saw and how the treatment there differs from the U.S. I found the lunch period another good time to network. It was rather difficult though for me personally to manage lunch because I have mobility issues and a cane and there were no tables to sit at. Because of this I ended up sitting elsewhere initially during lunch and then working to join conversations after.
I attended a breakout session devoted to “Imaging primary and metastatic ILC.” Breakout sessions ran concurrently and attendees could self-select which they wanted to join. There were approximately thirty attendees in this breakout session. The overall message was that imaging needs to be improved to be able to diagnose and monitor lobular breast cancer. It was interesting to hear from multiple people on the panel that there is also a shortage of radiologists, causing delays for patients. Patient concerns were shared with researchers and clinicians and among the top concerns were access to imaging, exposure to radiation, contrast exposure and difficulty with IV placement.
The second session I’ll summarize was focused on Tumor Microenvironment, specifically in Metastatic ILC. Here there was a presentation about circulating tumor cells (liquid biopsies) and how that may be a future way to monitor metastatic progression. There needs to be more research and clinical trials into liquid biopsies in various biofluids (beyond blood). This is an area that really needs more focus. Also discussed in this session was to promote research on misdiagnosis and delayed diagnosis in ILC as well as addressing patient-identified concerns through targeted research. I found those two discussions very interesting, and somewhat frustrating. It is clear we have a long way to go when it comes to diagnosing and treating metastatic ILC.
I’ve already had the opportunity to share what I’ve learned. I attended a metastatic breast cancer event the week after the Symposium and shared with other patient advocates what I learned. In addition, I’m the moderator for two facebook groups (one focused on lobular bc) and I shared some information already and will share more in the coming weeks. I also posted on social media during the Symposium, reaching several hundred followers. My hope is not only to educate but to prompt others to become ILC advocates in the future.
Hello friends and family! Welcome to fall (almost). The nights are getting cooler here and I’ve seen photos from others that the aspens are starting to change color in the mountains.
I write with good news. My PET scan of earlier this week shows that I’m stable. This is fantastic; it means that the cancer is not growing or spreading. The caveat is that lobular breast cancer sometimes doesn’t show up well on imaging. However, my blood tumor marker number dropped as well! The CA 27-29 gives an idea of how active the cancer is. A number of 38 or lower means the cancer is inactive. In mid-August it was 109. On September 11 it was 93! That was very welcome news!
The combination of the tumor marker dropping and my scan not showing progression means I can stay on the same treatment. I’m currently getting Enhertu every 3 weeks. I’ve got medications to deal with the side effects, overall I’m tolerating it very well.
I also spoke with my orthopedic surgeon this week. My recovery is going very well and he wished me a good time on my upcoming trip. He did mention several times how bad of shape my hip was in. I’m feeling grateful that I no longer have pain and hopefully I will be able to walk unaided soon. I still have some swelling and it’s hard getting used to walking since I’ve been using a cane for 2 years.
The symposium is 3 days long and the first day is focused on patient advocates. Maddy will come with me that day. The other 2 days are more research focused. We are excited to go and learn where research is headed for lobular breast cancer. My oncologist was not familiar with this conference and asked me to brief him on what I know. I’m more than happy to do that!
Not gonna lie – we are happy to go to Belgium as well. We should have one day where we can sight see. We will be in the city of Leuven which is east of Brussels. Watch for photos in the next blog post.
Life is good, right now for me life is great. I’m going to take it all in while also making sure I rest and don’t overdo it. Maddy may need to help me with that.