Adding a summary of my medications and milestones. Updated March 2026.
- Ibrance & Anastrozole: July 2019~June 2022 (Both oral meds; I tolerated them very well)
- Ibrance & Fulvestrant: June 2022~ June 2023 (Fulvestrant is a monthly shot; had slight progression most of the time I was on this combination)
- Clinical trial: June 2023-September 2023 (Phase 3 looking at Verzenio+Fulvestrant vs. Fulvestrant alone – I was in the control so was only getting Fulvestrant) I didn’t know if I was in the control or treatment group. I withdrew because I wanted to take Ibrance with the Fulvestrant. In September we discovered tumors growing on my spine – progression. Two surgeries to remove tumors from L4, L5 and T3.
- Xeloda: December 2023 (These meds did not work at all; discovered progression one month in – had hip pain and discovered new activity in my lumbar spine. I did NOT tolerate these meds at all. I felt terrible, like I’d rather die than take the medication.)
- Enhertu: February 2024 – March 2026 (Worked really well for the first 10 months and then mostly stable but with slow progression. Decided to stay on it as long as possible, finally the rate of progression increased. Tried to get into a clinical trial but the wait list was 10 people deep.)
- Verzenio & Tomaxifen: April 2026 (There is no clinical trial evidence that going back on a CDK4/6 inhibitor (like Ibrance) works, however, I know many with MBC who are trying a different CDK after the first one fails. We will monitor things closely and switch if it looks like it’s not working. We want to avoid progression getting to far along. Next treatment – if no clinical trials available – is likely to be Doxil. I’m going to advocate for another ADC (like Enhertu).)
2008 – 2020: The diagnosis and first year of living with MBC
I’ve written down my best recollection of dealing with breast cancer from a timeline and factual perspective. It’s probably not the most interesting read for most people. My reason for documenting it is three-fold. One, it’s cathartic to be able to put down in words all that has happened over the past 12 years for me as it relates to breast cancer. Of course this is one very small component of my life. Unfortunately, it’s become one that is most critical to my existence, but in the grand scheme of life we often forget the details of many events and experiences. It’s been helpful to capture it in one place and remind myself that I did nothing wrong. I did everything as ‘right’ as I possibly could for that particular time. Second, I really want to have a record of this for my kids. They see me in an entirely different light, as all of us see our parents. I know they will have a ton of questions about this and writing it provides some history they can reference. Third, I hope that others learn from it. I don’t really care what people learn, just that my going through this and sharing my story is not in vain. Maybe someone will be more compassionate to others struggling with disease, or someone might be inspired to advocate for equitable health care access, or a young person will stumble on it and be inspired to study medicine. Heck, I’d be happy if someone who reads this just simply has a conversation with a neighbor or friend about what stage IV cancer is and what it means.
Breast Cancer – Round 1 (2008-09)
I first dealt with breast cancer in 2008 and 2009. I was 39 in 2008 and so breast cancer was not high on the radar for any medical professionals. Then, and now, breast cancer is often thought of as a disease older/senior women get. In retrospect, I wish so much had been different then. I wish the medical team had told me more about the long term odds of it recurring. The first go-round was very non-urgent which was unsettling. There was no follow up, in retrospect it’s pretty disappointing to review the whole process. I believe everyone that treated me genuinely had my best interests at heart. I think that they may have been underresourced, or overworked or maybe the entire system was overwhelmed. It doesn’t really matter at this point – it is clear that our health care system was messed up then (as it is now).
2008 – summer
We ‘d decided to move to a new house in Champaign. We’d both finished our degrees and tried to get jobs together elsewhere, to no avail. We decided to make the best of the current situation and move to a newer, and bigger house. I noticed a small mass in my left breast at the beginning of the summer and didn’t think much of it, other than to remind myself to check it later. I promptly forgot about it.
November – We sold our house in September (3 days after the global markets crashed!) and closed on a brand new house November 10. Sometime in preparations for moving I noticed the mass in my breast was bigger. I called the ob/gyn and they ordered a mammogram. They said I had dense breasts (this would come back to haunt me and the exact type of breast cancer). They recommended I get an ultrasound, and then a biopsy.
Pre-diagnosis
December – By the end of December, I was told the mass I felt was benign based on the results of a biopsy. It was also large, in my opinion, something on the order of over 2.5 centimeters. I was told since it was benign I didn’t need to do anything, just get yearly mammograms. I insisted they remove the mass. They argued against it, but I did not budge. The oncologist agreed to remove it but said that if we were going to do surgery, we should get an MRI of my breasts first to make sure we don’t miss anything else.
I had an MRI just after Christmas that showed a second mass in my left breast, back up against my chest wall. There is no way I’d ever feel this mass through a physical exam. The oncologist said it was not urgent and that we’d get things scheduled after the holidays were over.
Early March – I’d still not heard back from the doctors by February and started calling for an appointment and information. My only recollection is that it took like what seemed forever to get an actual appointment. When I finally got in to see the oncologist (Dr. Rowland at Carle in Urbana, Illinois) he seemed surprised that I didn’t have an appointment sooner. It was clear I had fallen through the cracks.
I should add here that during December and January Glen and I both got job offers in Boulder, Colorado with a negotiable start date. So, in the midst of all this and working full time (with 2 and 5 year olds) we negotiated job offers and put our brand new house on the market. Oh, and I had a pre-job trip to Geneva, Switzerland in an attempt for them to convince me to take the job. We planned to move to Colorado the end of June, right after Glen finished an 8-week field campaign for work. (BTW, the first half of 2009 sucked in almost every way, nothing compared to the second half of 2019 though.)
Surgery and diagnosis
The doctors recommended they do an excisional biopsy. This means they do surgery to remove the mass and then do pathology testing on it to see what the deal is (benign or malignant (cancerous)). The results came back that it was pre-cancerous (stage 0) and that I had both DCIS and LCIS. The “IS” means ‘in situ’ (in place) so it hadn’t spread, which was very good news. Of note, I got the news via phone while I was on travel (to Boulder, CO). I took the call in a hallway and finally found an empty room to sit down in. This would not be the first time I got bad cancer news over the phone when I was not in my home state.
DCIS is ductal carcinoma in situ – this is cancer that forms in the ducts of the breast. LCIS is lobular carcinoma in situ, cancer that forms in the milk glands (lobules) of the breast. Lobular breast cancer is not common. (In the About MBC page I share more on the difference between lobular and ductal and why it matters.)
More importantly, for the the mass that was near my chest wall they were not able to get clean margins from the surgery. This means that at the outer edge of the mass they removed there were cancer cells. This could mean that there are still cancer cells that are in the body. So, another surgery would be necessary. The surgeon recommended another excisional biopsy. I opted for a mastectomy. (I’m not a busty person to begin with and after the first surgery there was not much left to work with and I couldn’t see how there was any other choice.) During this entire time Glen was supportive, by my side, and researching everything he could about the situation and what we should do.
In late March (over spring break – yes, I scheduled my surgery around my work schedule) I had a single mastectomy. It sucked. It was hard on every level (recovery, dealing with a 5 and 2 yr old, having to go back to work). The surgery itself went fine and the medical team was satisfied.
I asked what next…radiation? Tamaxofin (hormone therapy)? They replied “nothing”. You are done. You are cured. Go on with your life. They suggested that once I got settled in Colorado to establish myself with an oncologist. I did that and the oncologist also basically said “Nice to meet you. Glad everything is taken care of.”
The common statistic everyone quotes with breast cancer is that if you make it through 5 years post-treatment without a recurrence you are cured. That is wrong. Absolutely, positively wrong and bad information. 20 to 30% of ALL breast cancers return and become metastatic – stag IV – incurable. Why everyone believes that once you are past a 5 year mark you are not likely to have to deal with it again is mind boggling and frustrating.
That was it. I was “cured” and everyone behaved as if I should go on with my life like nothing had happened. I pretty much did, until 10 years later.
Breast Cancer Revisited
2018
Hindsight is 20/20 – truly. In the fall of 2018 my back started bothering me. Nothing major, just kind of achy in my lower back, hard to get comfortable – that sort of thing. I typically get up earlier than anyone else in the house and one morning I bent over to throw something in a small trash can and almost fell to the floor. I felt something slip or slide in my lower back. It felt very odd. I was able to stand up and walk to the sofa. After that I noticed my back aching now and again but didn’t think much of it.
2019 – Pre-Diagnosis
February – My back gave out on me again, this time in the shower. It felt like last fall where something slipped in my lower back. I knew to be careful and managed through the discomfort.
Spring – By mid-April my back was really bothering me. I went on an all day job interview (awesome opportunity that I had to pass on, thanks cancer) and came home that evening barely able to stand, my back hurt so bad. I couldn’t get comfortable, standing, sitting, nothing. I laid down on the living room floor. That provided a little relief but I couldn’t move. Literally could not roll over or move – the pain was unbearable. I had some oxycotin left over from my ankle surgery and took some. Once that set in, Glen was able to pick me up. It was so painful. The following morning I went to the ER.
In the ER they took x-rays and found nothing. They instructed me to see my general practitioner. I went and he basically said “Well, you are middle-aged and with time our spine compresses and you are probably just having the start of back problems. Exercise, eat well, etc.”
I basically learned how to manage the pain and how to be careful with moving so as to not trigger anything. Honestly, I didn’t think much more about it. Who doesn’t have aches and pains as they age? Most of us are not the type of people to get a pain and immediately think “I’m dying.”
I also was not feeling well generally. I had a lot of travel for work in March and April and figured I was running myself down. I cancelled a few trips. I vowed to really kick it in to high gear to take better care of myself, that I had to get my act together. I was exercising more and yet when I’d look in the mirror I thought “you look terrible” – my face looked drained and just not right. I made appointments for everything – eye dr., dentist, mammogram, ob/gyn, etc.
May – A mammogram came back with a request for a biopsy. I was a little alarmed but not overly. Over the past 10 years, approximately every other mammogram required me to get an ultrasound. Each time they said they were concerned about how something looked and then every time I had the ultrasound they said “it was nothing”. I figured this was going to be the same. The mammogram I just had showed many microcalcifications that showed up and given my history needed more examination. (Microcalcifications can be a signal of bigger problems.)
June – I had the biopsy just before my birthday at the end of the month. I got the results on a Friday when I was in DC on travel. The doctor called and said I needed to see a surgeon asap and gave me three to call. There was an urgency in her message that shook me. I managed to get an appointment with one the following Monday, July 1. The plane ride from DC to Denver felt like one of the longest of my life.
July – July 1: Glen went with me to the surgeon (Dr. Fox). He did an exam of my right breast and we talked about how he was recommending a mastectomy given my history. I was not excited about it having gone through that already. We spent a fair amount of time with him talking about my situation and what he thought I should do. He asked to examine the other side. I said of course, there is nothing there. He did a manual exam and found a mass up where the breast tissue would have met the armpit. He pulled out the ultrasound and Glen and I watched the screen. It showed a huge mass with a lot of blood flow to it. We all knew what that meant without saying anything. The surgeon was very concerned and asked me to come back the next day for a biopsy of the mass.
July 2 – I went back at noon to the medical building for the biopsy. The dr. was in surgery at a nearby hospital and expected to be back shortly after noon. He got delayed and didn’t make it until close to 3:30. Interestingly, he kept calling his office telling the staff to ask me not to leave. He would come as soon as he could. When he got to the office he had two interns assist with the biopsy. It was *really* hard for him to get the needle into the mass. Like, really hard. It was almost like it was a solid, rock mass. I remember tears rolling down my face it hurt so bad. He was determined and once he got what he needed he said he’d ask for an expedited analysis. (I enjoyed a massive bruise for over a week.)
July 3 – Dr. Fox called me around 6 pm and told me the pathology came back as Invasive Lobular Carcinoma. He was said he’d already contacted an oncologist at the Cancer Center in the medical complex and had put in a request for a PET scan. He said it was important to know the extent of the disease so they knew how to treat it. I was with the girls at the time he called, they were getting hair cuts. I took the call outside on the sidewalk. (See the theme? bad news when I’m not home.) Glen and I took a long walk that night to talk without the girls around. I think it’s fair to say we were both terrified.
July 11– I contacted with my ob/gyn and she helped me switch to a different oncologist (Dr. Andorsky) who I preferred to see. Glen and I went to see him on the 11th. He explained what the likely chemo course would be – intensive chemo every 3 weeks, likely 6 to 8 rounds. He wanted to wait until the results of the PET scan though to make sure we were doing the right course of treatment. He also was waiting for more detailed information about the pathology – it would help determine the course of treatment. We went to lunch afterward and I just remember I couldn’t eat. Glen was researching the various types of chemo and effects and so forth. I’m so grateful for his pragmatic approach and that he can do the research and then share with me. I was in no state of mind to read more detail.
That weekend we were traveling to Wisconsin for some family events. I’d told my sisters what I knew but we kept things on the down low because (1) it would be a distraction from the other events and (2) we didn’t have concrete information yet. There is no point in getting people worried when we didn’t know what to worry about. In preparing to leave for the trip, I mowed the lawn. Pushing the lawn mower apparently aggravated my back terribly. I could barely move; it was similar to when I went to the ER. Needless to say that was the last time I will ever mow a lawn in my life!
Even though the medical team wanted to do a PET scan right away, it doesn’t work that way here in the U.S. Any procedure has to be approved by insurance (if you are lucky to have any). The insurance company has 5 days to reply to a request for approval of a procedure. 5 days just to approve it. After the approval then you have to get on the schedule to actually get the procedure. After that you have to have the results read and sent to your doctor. At this point we were in Wisconsin visiting family. I recall sitting on the Terrace at UW-Madison having a beer while the girls ate ice cream and begging with the scheduler to get me on the books asap. I managed to get a PET scan appointment for July 16.
Over the next two weeks Glen would be running a national workshop that he had been leading the planning of for over a year. It had been a huge amount of work to coordinate and we’d known for a year that those two weeks he was going to be consumed with work and running this workshop. We’d actually planned much of our summer around these two weeks knowing what a heavy lift it would be for him.
July 16 – I was able to get a PET scan. I was not nervous in the way you’d expect. I honestly did not expect to have the results be ‘bad’. The scan itself went fine. I didn’t have any reaction to the contrast. The waiting was hard. After the scan I met briefly with the nurse navigator – someone whose job it is to help patients figure out what to do next, how to get help, etc. She said she’d hold time on her calendar for me on the 18th in case I wanted to talk after getting the results of the PET.
Diagnosis
Knowledge is power. Once we know things, we can figure out what to do with the information – good or bad, or perhaps nothing at all. If you have knowledge though, you have the ability to act.
July 18 – I met with my oncologist (Dr. Andorsky). Glen was running his workshop so I went alone, which was fine. He started with pathology news, that it was hormone positive (estrogen and progesterone positive). This allowed for more treatment options. He then said “Unfortunately, it’s spread to your bones.” That means there is nothing they can do that will cure it. The cancer had gone out of control and was trying to invade my body. I was stunned, of course. I hadn’t expected to hear that. He showed me a 3-D image of my PET scan and where the cancer was (ribs, hip, back). This certainly explained the back pain I’d be having for almost a full year! He then explained there were medications I could take that might stop the progression, that there are options for keeping it in check – options that weren’t around 10 years ago when I had my first encounter with breast cancer – that there were treatments that might make it more like a chronic condition rather than a terminal disease.
I immediately switched into the mode of “Ok, let’s do this. Let’s find the right medication and treatment that we make this a chronic condition. He said the meds he was prescribing were working very well for many women. I asked how long they’d work and he couldn’t say. He did have some women who had been on it for 4 years and were doing fine. Four years didn’t sound like very long. I have plans! I need a couple more decades! The good news is that the medication was only FDA approved in 2015 – so this means that those women who’d been on it from the start were still doing well. They don’t have more than 4 years worth of data. He said I could start the medication after I get a tutorial from the nurse. That would be scheduled for Monday and then start the meds Tuesday, July 23.
I didn’t cry then in the office, just me and the oncologist. I choked up a bit talking to the doctor but really just tried to remember what the next steps were. I texted Glen. I don’t even recall what I said, probably something like ‘it’s not good’. I went down to the nurse advocate and in talking with her was overwhelmed with emotion. It was very good to have the option to cry in a room with the door closed. She was so helpful – she said I needed to tell Glen to come now to be with me. She explained what support group options there were. She gave advice on how to talk to the girls and how to reach out to the adults they interact with on a daily basis.
Glen and I sat on the outdoor patio of the Cancer Center and didn’t say a lot. Just trying to wrap our head around all this. We’d come in different cars. At some point he left (not sure if he went home or to the workshop, home I think). I recall sitting in my car calling my family and best friends. I couldn’t make those calls from home because the girls were there and we wanted to wait and figure out how best to tell them.
We talked with the girls that night. We took the approach that this was a family situation and we were going to deal with it as a family. Things would change a little to make sure that I was able to manage this as best as possible for as long as possible. They knew I had been going to the doctor a lot and that it was related to cancer. We didn’t want to worry them before this point. We only talked with them once we knew exactly what was going on.
In the conversation with them we explained that the cancer had come back. I had a very bad diagnosis but that we were going to figure out how to deal with it and that we have every intention of being successful. We reminded them that we are scientists and approach things with logic and evidence and that was a good thing. We pointed out that we were able to diagnose Evelyn as having Rumination Syndrome – after her seeing multiple experts at Children’s Hospital and having numerous procedures. We were the ones that figured it out. If we can do that, we can figure this out.
We did talk about how there is no cure. That was not good but it didn’t mean I was going to die tomorrow. We used Ann’s situation as an example. She is living with a condition that requires her to take medication every day. I would be the same. That made sense to them.
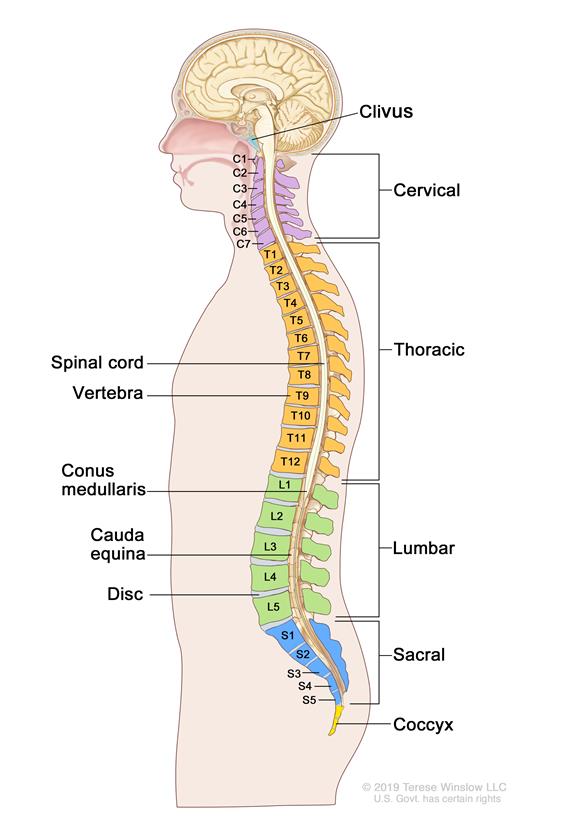
More details of the diagnosis. – I have Invasive Lobular Carcinoma. It has spread (metastasized) to my bones. There was a mass between my left armpit and where my breast was. That was the only physical evidence of the disease. The breast cancer went through my lymph nodes and into my blood stream. The cancer took up residence in my pelvis (hips), ribs and spine. Bones are one of the more common areas for breast cancer to migrate to. (Lungs, liver and brain are the others.) I do not have bone cancer. I have breast cancer that has migrated to the bones. It is treated as breast cancer. Once cancer leaves the breast area it will take over a body. At that point, the only option is to control the spread (ideally stop it).
More specifically, the areas of the spine impacted include C7, T9, T10, L4 and S1. At least this explains why I had so many issues with my back! This image is from https://www.cancer.gov/publications/dictionaries/cancer-terms/def/spinal-column.
2019 – Treatment
July 22– Glen and I went for a medication tutorial with a nurse. She explained the four meds I would be on/receive and how we needed to deal with them. Honestly, it was kind of scary the way she described it. Gloves, all the precautions, etc. In reality, it’s not that bad to deal with (I can say this after 11 months on the meds).
July 23 – I went to the infusion center at Rocky Mountain Cancer Center. It’s literally 5 miles down the street from our house. I received an infusion of Zometa. It’s a bone strengthener that almost immediately reduced the pain in my back. The infusion is only 20 minutes. I also receved a shot of Lupron. The Lupron induces menopause. In order for the medications to work they needed to stop the production of estrogen. I also got my oral medications of Ibrance and Anastrazole.
The Anastrazole is a “nonsteroidal aromatase inhibitor” – it basically stops the body from producing estrogen [Science lesson: Aromatase is an enzyme that is involved in the production of estrogen. It basically allows for testosterone to covert to estrogen. Women do produce small amounts of testosterone in ovaries and adrenal glands.] So, an aromatase inhibitor is something that stops the production of the aromatase. I take Anastrazole orally every day, along with Ibrance.
Ibrance is the primary medication – one capsule once a day (meds for 3 weeks and then 1 week off). By design, it goes into the actual cancer cells and stop them from reproducing and possibly kills them. (F-ing amazing! Yay science!) It doesn’t work for everyone and it won’t work forever. We were hopeful that it would work (and it did as evidenced by scans in October). Ibrance is some amazing stuff. It’s crazy really that modern medicine has developed such a sophisticated medication. I’m grateful that researchers and pharmaceutical companies have invested time and money into this. (I do wish they did not make such an astronomical profit off of it. (Small or modest profit would be ok. That topic is for another time, I could go on and on….)
So, my first line of treatment is: Ibrance and Anastrazole orally, daily combined with once per month infusions of Zometa and a Lupron shot. I see the oncologist monthly (on treatment days). Every three months I have scans to see if the medication is working or not. Once the treatment stops working we look for the next option. Of course, at some point you run out of options – I’m not willing to get to that point anytime soon.
May – I’ve been very fortunate that after 11 cycles (months) of treatment I have very few side effects, all of which are minor. Side effects vary widely by person. I generally considered myself healthy most of my adult life – eat well, mostly plants, regular exercise, no sugary drinks or fast food. I do drink wine – and love it.
I keep a daily journal (thank you science training) and that’s allowed me to monitor side effects and identify patterns. This, in turn, helps me manage expectations and adjust my diet, exercise and sleep as needed.
As of the end of May (2020) I am stable. The cancer progression has stopped. The medications are not allowing it to spread. We know this from a bone scan and CT scan. Every three months I will get scans to check the effectiveness of the medication. When this treatment line stops working (the cancer spreads) then we go to treatment line #2 (TBD). Let’s hope that’s not for a long time.
