Hello again. A quick update on where I’ve landed with treatment.
Over the next 2 weeks I’ll start what I consider my 5th line of treatment. If you are interested I’m tracking my treatments on the My Story link of this website/blog.
I say 5th because I’m not really counting the clinical trial I was on. It was a blind trial so you don’t know if you are in the treatment or control group. After the fact I learned I was in the control group so I was really getting the same treatment as before the trial. Anyway, it’s not always straightforward to track treatments.
Speaking of clinical trials – I was hoping to get in to a Phase 2 trial with a “new” drug. Phase 2 trials have limited participation and the focus is to figure out the right dosing. The trial had a wait list of 10 women and the wait list was “not moving”. Sigh. A disappointment.
I’ve decided to try another drug similar to one that I was on before (from the same “class” of drugs). My oncologist says that in his experience he’s not seen great results from doing this. However, I’m seeing more people with MBC (metastatic breast cancer) who are doing this, some with good success.
So, he agreed that we will try it and closely monitor things through bloodwork and how I’m feeling. I’ll have another scan in early June to see if it’s stopped the progression.
I’m going to take Verzenio (Abemaciclib) with Tamoxifen. Fortunately for me, when I had early stage breast cancer I didn’t take any medications. This means they are all an option for me now (#silverlining). Many women with early stage breast cancer take Tamoxifen for 5 or 10 years as a way to prevent the cancer from returning.
Verzenio is a CDK 4/6 inhibitor (and has to be taken with something to knock down estrogen – the Tamoxifen in this case). When I was diagnosed in 2019 the “preferred” CDK 4/6 inhibitor was Ibrance. Since that time, research studies have shown that Verzenio is actually a bit superior. My oncologist told me that if I were diagnosed today he’s put me on Verzenio.
So, we will give this a try. They are both oral medications (nice, I don’t have to go to the cancer center). Verzenio is known to cause GI issues, in some cases severe. I have tolerated most of the drugs really well and am hoping this is the case again.
Am I nervous? Yes.
Anxious? You bet.
Optimistic? Absolutely!
In the meantime, life continues! Maddy and I just got back from a week in Rome. Evelyn and I are planning a trip to Europe in May. Hopefully I’ll be well enough for Glen and I to do a trip in early fall. I’m going absolutely nowhere in April and will be hitting the trails to walk and soak up the beautiful Colorado views! Come visit, I could use walking partners!
Onward!
My last Enhertu infusionTrevi Fountain, RomeSo many people!Roman ForumRoman Colosseum
Happy spring! It’s been crazy warm here with basically no snow this winter. It’s made it a bit easier to get outside but also worrisome.
Christmas in March – Glen and the girls got me a stained glass making class for Christmas. You can see how beautiful the weather looks!
One thing I try not worry about is this damn cancer. There is a lot about my situation that is out of my control. Sometimes it’s hard not to worry and in those cases I only give my self a set amount of time and then I put the worry away.
It’s been a wild three months.
🌷 Radiation to my C1 last fall looks like it was successful in stopping that cancer lesion.
🌷 I was taking a walk in January and my hip/femur (greater trochanter) fractured. It was minor and no longer hurts. Still, walking may = fracture.
🌷 This week I had 5 doses of radiation on that fracture to try to knock down the cancer and reduce any further fracture.
🌷 This week I had a total of 8 medical appointments (5 radiation, a PET scan, an oncology visit, and an echocardiogram).
🌷 PET scan results were not great. Looks like the cancer has gotten a bit more active. Looking at changing treatments.
As you’ve probably learned from me by now, there are a finite number of treatments. Once those run out there is nothing to stop the cancer.
How many treatment lines are there? It varies for each person depending on your cancer subtype. Exact number is unclear (but not a huge number, maybe 6-10ish?). The positive side is that research and clinical trials are making more drugs available all the time. The drug I’ve been on for the past 2 years was not an option for me when I was diagnosed! I just need more drugs to become available and approved!
I don’t know what I’ll do for my next reatment line. We are looking at a clinical trials.
Please, please, talk to your fiends, family and neighbors about how important it is for the federal government to pass budgets on time and to fund cancer research! I know several promising trials that have stopped because of all the nonsense going on with the budget and NIH. It’s not partisan, it’s life or death for some of us.
All of this being said, I’m optimistic that I’ll find a good next treatment and hope that the side effects will be minimal and it will be very effective.
In the meantime I’m doing all the things! So far this year I’ve taken ballet classes, a sketching class, Spanish lessons, signed up to work with a personal trainer and am looking into learning to knit. I have a few trips planned with the girls and will enjoy every single day.
Wishing you all a fantastic rest of March. I’ll share more when I know it.
I was in Kansas City for work and caught the Univ. Colorado Women’s BB tournament game!Nancy came for weekend and we had an amazing time!Went to see Maddy perform with her dance group.Phoenix for work and Glen joined me for the weekend.Got to see my bestie (Laura) briefly.
The Summit included a day of education about MBC as well as how to advocate for various bills and funding.
Tuesday we marched (with police escort) from our hotel to the Capitol. We had a remembrance on the grass. I am holding the sign on the end, near the last “R”. We spoke the names of those who have died from MBC (and I included my aunt Jeanne Moretti as well as several other friends who have passed).
Policy advocates preparing to visit with Congressional staffers.
We met with staffers of our elected representatives. Staffers were taking meetings even though the House was not in session and the federal government was/is closed.
Staffer from Rep. Joe Neguse’s office.Staffer from Senator Bennet’s office.
There were four “asks” that we made. I had fantastic interactions and felt like I was heard. I’ll share here what those asks were – if you feel compelled to share with friends/family or to reach out to your own elected representatives that would mean a lot.
Did you know that if you have MBC and need to stop working there is 5-month waiting period for Social Security Disability Insurance (SSDI) benefits to start? In addition, after that there is a 24-month waiting period before you are eligible for Medicare! I am one of the fortunate people who is living longer with my MBC diagnosis and can still work. Women with different subtypes have a prognosis of 2-3 years. During this time they can’t work and can’t get SSDI or Medicare. House bill 2048 “Metastatic Breast Cancer Access to Care Act” would eliminate the waiting period.
Did you know that where you live impacts how private insurance pays for MBC drugs? Private insurance treats medication received at a cancer center different from medication taken at home. Recall that I was on a pill (Ibrance) for the first 4 years. I live in a state where private insurance is required to pay for this (chemo) regardless of how it is given: intravenous or a pill. House bill 4101 (Cancer Drug Parity Act) would require private insurance to cover oral cancer drugs the same as IV drugs, regardless of what state you live in.
The U.S. is the largest funder in the world of cancer research. The administration’s budget zeroed out some breast cancer research programs and greatly reduced funding for the National Institutes of Health (NIH). Fortunately, Congress likes science – we asked them to provide the NIH with the same funding as last year and restore the breast cancer program in the Dept. of Defense.
Did you know there is a national database of incidence of cancer? It was created in the ‘70s during the Nixon administration. Unfortunately, it has not been updated since then. The Surveillance, Epidemiology and End Results (SEER) database provides information on cancer statistics which is used to inform where research dollars should go. It needs to be updated badly and I asked our reps to support funding for it. SEER help us understand where there is a high burden of cancer. It turns out that not every state is contributing to it. In addition, it does not include any recurrence of cancer. When I was first diagnosed, my information was put into SEER (LCIS and stage 0 DCIS breast cancer). However, there is no mechanism to update my information! According to SEER I was treated in 2009 and all is good with me. As you can see, the number of people with MBC or with any recurrent cancer are not counted which means we have no idea who is living with metastatic disease (unless you were diagnosed with MBC right away, which is only 6% of all MBC diagnoses).
That was a lot! If you are still reading, thank you. If you’d like more information about anything including language to send to your elected representatives, shoot me an email (charlevo@gmail.com).
I have one other cancer event this week and then I will take a break from cancer the rest of this month. I hope you are keeping balance in your life as well.
September was a busy month for me in managing cancer.
Back in June I had a brain MRI, which includes the very top of your spine (cervical). At that time, it looked like there might be an active tumor in part of my C1 vertebrae. I also had a full body PET scan that showed “stable” cancer at the time (mainly my spine has been problematic).
The stable PET scan means that my treatment (Enhertu) is largely working. However, the tumor on my C1 made me nervous. Your C1 is directly at the back of your head at the height of your nose. If anything goes wrong there it can be complicated and in the words of my oncologist “catastrophic” 😳
After discussing with my oncologist in August, we decided to radiate it. It’s not uncommon with metastatic breast cancer (MBC) to consider radiating smaller tumors if everything else is stable or no evidence of disease (NED).
So, I decided to pack this in to September which was already busy.
After another MRI of my cervical spine I met with a radiation oncologist. He wanted to do Stereotactic external Beam Radiation Therapy (SBRT) – a concentrated radiation that would have been 2 sessions.
My insurance company disagreed with my radiation oncologist and wouldn’t cover it.
I could appeal it but that can take weeks and I didn’t want to give the tumor more time to get comfy and grow. So instead, I had to go for 10 sessions over two weeks.
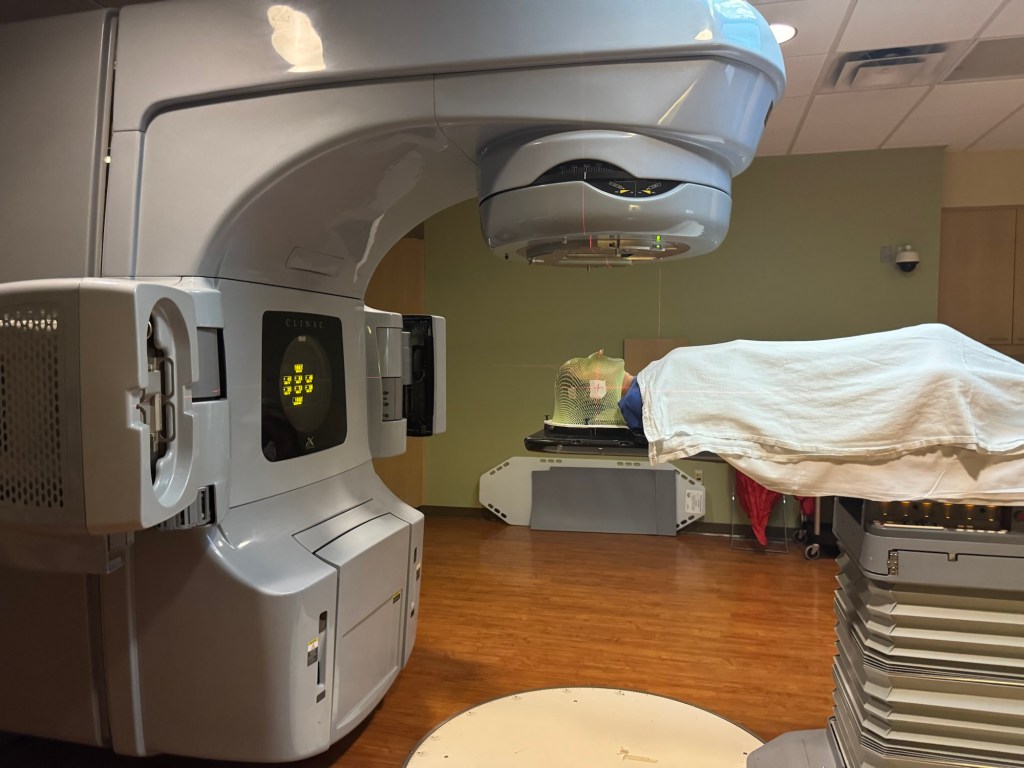
You have to lay perfectly still for radiation so that the beam hits the intended target. At my planning session appointment they created a mask. A mesh of warm plastic was placed over my face and head and molded to my exact shape. The photo of the mask shows me with a big smile – not that I’m super happy to be doing this, I just naturally smile for photos.
A spanking new mold of my face and head.
Then I got out of town. Drove Maddy to Cal Poly and then back home. The next day I jumped on a plane to Providence for work. Glen flew out at the end of the week and we spent the weekend (our first as official “empty nesters”) with my cousin playing tourist.
Beautiful fall weather made a boat tour of light houses on Naragassent Bay just delightful!
We got home late on a Sunday and Monday morning at 9am I had my first radiation treatment.
The photo shows me right after they finished a treatment. The mask mostly feels like a heavy blanket with a lot of holes draped over your head.
The mask is literally snapped to the table. You can’t move your head at all. You can kind of see through the holes and of course you can breathe. The round equipment above my head rotated all the way around the table that I’m lying on.
I had 10 treatments (M-F) over two weeks. Within those 2 weeks I also had my Enhertu infusion and got my flu and COVID boosters.
As soon as I finished radiation I headed back to the east coast, Washington DC this time to advocate on the Hill for funding for cancer research.
It’s been a lot, however, I refuse to let cancer dictate my life. Most of those days I was in bed before 9pm. I’m grateful that my side effects are minimal and I can still do “all the things”.
The side effects of radiation to your head are not pleasant. This week I developed a wicked sore throat to the point that I couldn’t swallow. Food doesn’t taste like anything. My fatigue has been ridiculous.
October is a little more quiet but more travel for work and fun.
I hope you all are living your best life and doing the things that make you happy and matter to you, whatever that might be.
Onward!
Our last family dinner before Maddy left for college.Saying “see you later” to MaddyTouring in Rhode Island – this is the homestead of the painter who did the portrait of George Washington that was the inspiration for the $1 bill
When we moved to Colorado 16 years ago and I went to get my car license plates updated, I was asked if I wanted a “specialty plate”. There was one for breast cancer and I had been diagnosed only 6 months earlier.
“What does the extra $60 for the breast cancer specialty plate go toward?”
Clerk: “Um, I don’t know I think it’s just so you can raise awareness.”
“No thanks” – hard pass! They were collecting money that in no way went towards breast cancer at all.
Today is the start of Breast Cancer Awareness Month (BCAM) and you will see pink everywhere. I think it’s very important for people to be aware of cancer. However, at this point I’m pretty sure everyone in the U.S. is aware of breast cancer – how can you not be when you are confronted with pink at every turn!
Any business – or person – can “support” BCAM and do whatever they want with any money they might raise or collect.
Before you “round up” your groceries for BCAM or donate to a fundraiser, find out where that money is going.
If you are inclined to financially support BCAM, consider focusing on organizations that support scientific research of breast cancer. Scientific research is how we get treatments and how we understand how exactly breast cancer behaves. (Spoiler alert: we still don’t know how breast cancer behaves.)
Charity Navigator is a great resource to see how organizations use their funds (administrative costs vs. programming).
My favorite organizations focus on research mainly for stage 4 breast cancer (Metastatic Breast Cancer, MBC), they are listed below. Did you know?
Stage 4 (metastatic breast cancer MBC) is the ONLY breast cancer that kills.
30% of people “cured” from early stage breast cancer will eventually have a recurrence as Stage 4.
MBC is a terminal diagnosis.
If we cure stage 4, we cure everyone. Full stop.
If you’d at least share some of this information with one other person that would make me happy beyond belief.
We need more breast cancer research and especially stage 4. My life and the lives of my MBC friends depends on it.
It’s been a bit so a short update here. Short version: currently stable, minus a pesky tumor in my C1.
I had a PET scan earlier this month. I met with my oncologist today and the imaging didn’t show any change. I’ve been feeling pretty well lately so that is a good sign. My tumor markers keep climbing which is worrisome but there is no evidence prompting a change in medication since my imaging doesn’t show anything. I’ll continue on Enhertu for the next 3 months.
I do have a tumor in my C1 and compared to June it’s a bit more active. It’s possible that this is the reason for the rising tumor markers – it’s hard to say. I’m having radiation on the C1 (started today). More on that later.
Overall, I’m trying to stay active and have balance in my life. I think that’s hard for all of us, cancer is just one more thing to navigate.
We are officially in fall – hopefully you had a great summer and fall is off to a good start.
Onward!
Grateful for walking paths from the cancer center. I took a walk before my appointment today.
This month marks my living with metastatic breast cancer for 6 years.
Six years with a terminal illness.
I’ve been reflecting a lot this month both on this unwanted journey and life overall. I’ve had the privilege of:
2,190 days including sunrises and sunsets
312 weeks
72 months
6 years
And that included:
1 Hospitalization
2 Support groups I created
4 Lines of treatment
6 Cancer related surgeries
7 Cancer related conferences attended
50+ Scans of my body or parts thereof
106 Blog posts
150+ Doctor appointments
170+ People connected with in support groups I started
That is a lot of cancering! There have been highs and some very low points. Fortunately, my cancer only got somewhat out of control once. For the most part I’ve been fortunate to tolerate medications well, have minimal side effects, and be surrounded by an amazing medical team and an incredible new group of friends I’ve met because of cancer.
As you all know, cancer is but one part of my life, even though this blog is cancer-focused. I’m proud of all I’ve accomplished over the last 6 years. The big moments and the small ones too. Every moment adds up to life. It wasn’t always easy, but who ever said life was easy?
Some highlights:
1 Global pandemic
2 Countries visited
4 Graduations attended
5 Colorado weekend getaways
6 Nutcracker ballet performances attended
13 States visited
30+ Visitors here to Colorado
34 Trips in the U.S.
? Meals out with friends = too many to count
I will never say that cancer is a gift.
Cancer also did not change the way I live my life and how I prioritize. I was already doing that just fine thank you!
It has pushed out opportunity to do some things and so the choices I make on how to spend time is especially important.
I hope you reflect on your last 6 years and find it filled with amazing experiences, wonderful people, and quiet moments.
Onward to the next 6 years!
A few photos from the first 6 years of living with MBC –
Winter walksFirst concert at Red RocksHoliday family photoFlorida family visitorsWedding anniversaryGo Pack Go!Best FriendsChristmasGo Buffs!Evelyn graduationMaddy graduationFamily in the mountains55-5 partyEast coast familyHawaiiMy heartSunset walksInfusion room
No, this is not all about Toulouse, but it could be! He’s such a good little furry guy!
Toulouse ❤️
In case you are interested, I’m summarizing how a PET scan can help us monitor metastatic breast cancer. If you are not in a science-y mood, you might want to pass on this post.
A PET (Positron Emission Tomography) scan is often used to detect cancer. It is also commonly used to diagnose heart disease and brain conditions. With cancer it is used to determine if the cancer has spread to other parts of the body (metastasized). [Tomography = a technique for displaying a representation of a cross section through a human body or other solid object.]
A PET scan detects cellular changes in organs and tissues earlier than CT and MRI scans. The scan is painless, although sometimes people can feel claustrophobic as their head moves through the large tube. The machine used to do the scan is shown in this diagram from the Cleveland Clinic.
Machine used for PET (and CT) scans (image from Cleveland Clinic).
Prior to the scan, an injection of a glucose-based radiotracer is given. A person has to wait about 45 minutes after the injection before the scan is started. This gives the radiotracer time to circulate through the blood stream and body.
A PET scan can take 30 minutes to 2 hours depending on what exactly is being examined. The radioactive tracer allows the machine to detect diseased cells. Diseased cells will uptake (or collect) more of the glucose radioactive tracer because they are more metabolically active than healthy cells. This increased uptake is visualized as brighter spots on the imaging.
The most common radiotracer used in PET scans is fluorodeoxyglucose (FDG). Once it’s inside the cell, it’s trapped. The PET scan machine can quantify the amount of tracer uptake using SUV. SUV (Standard Uptake Value) is a quantitative measure used to assess the concentration of the tracer.
SUV represents the ratio of the amount of radioactive tracer in a specific region of interest (like a tumor) to the amount of tracer that would be expected in a similar volume of normal tissue, taking into account the injected dose and patient’s weight.
Changes in the SUV number over time can help determine how well a patient is responding to cancer treatment.
In an imaging report, SUV numbers are reported. The radiologist or oncologist can then compare the SUV numbers to previous PET scans to determine if the cancer is more active (higher SUV number) or less active or inactive (lower SUV number).
While all of this sounds very concrete and specific, it’s still just an approximation of what is happening in the body. Results from a PET scan are used along with other factors such as how an individual is feeling, whether or not there is pain present, and blood work results.
PET-CT
Sometimes a PET scan is done in conjunction with a CT scan. The same machine does both of them and a patient would have both done during the single scanning session. The combination of both a PET and CT scan produces a three-dimensional image that allows for a more accurate diagnosis.
A CT scan is Computed Tomography and uses x-rays to get a detailed view inside the body. It produces still images of organs and body structures (such as bones). Sometimes it’s referred to as a CAT scan – it’s the same thing. CAT = Computed Axial Tomography.
Instead of creating a flat, 2D image, a CT scan takes dozens to hundreds of images of your body. To get these images, a CT machine takes X-ray pictures as it revolves around you.
After a scan is completed, the technician makes sure the images look ok and then it is sent to a radiologist to interpret and read. The radiologist writes a report of what they see, ideally comparing it to previous PET or PET-CT scans. That report is then forwarded to the oncologist and the patient. The oncologist and patient, together, determine what changes to make to treatment (or not) based on the scan results as well as other factors such as how the patient is feeling and blood work.
Happy summer my friends. In Colorado we are starting off with a cool, wet one which is great for the a/c bill but less ideal for exploring outside.
Lot’s going on here including medically.
I had some work travel last month and towards the end I started not feeling well, including being light headed. I mentioned this to my oncology nurse 2 days ago during my treatment appointments and she scheduled a brain MRI and echocardiogram. Yes, light headedness triggers the immediate thought of brain metastasis.
Recall from my last post that we’ve found the MRI to be the best imaging for me. The brain MRI captures the head and top part of the spine (cervical). Mixed results: no brain metastasis 🙌 but it did pick up a new lesion on my C1 vertebrae 👎.
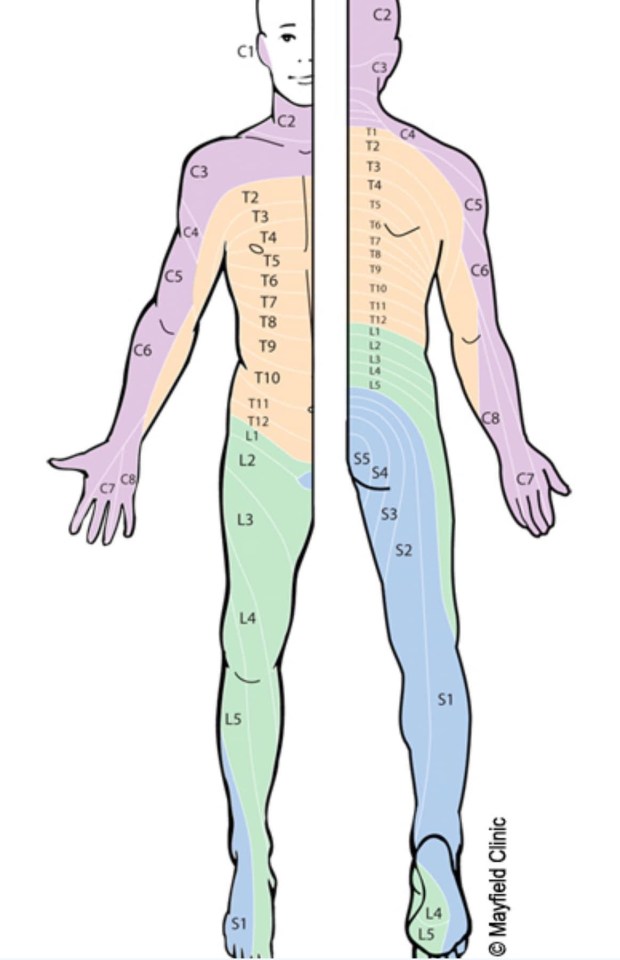
The nerves that come out of the C1 impact the sides of your face and head as shown in this nifty diagram (one of my fav diagrams BTW).
The most likely explanation for my light headedness is that the lesion (tumor) is pressing on the nerves. So, my oncologist has ordered another PET/CT to check again. It seems a little insane to keep getting imaging that doesn’t work so well – I guess he wants to confirm or look for other lesions.
My tumor markers did drop the end of last month which is in contradiction to the new tumor.
See how complicated and tricky cancer is?
For now, I’ll get the PET/CT and an echocardiogram and keep doing all the things (eating healthy, moving, relaxing) and we shall see where this takes me.
After my work trip I spent 2 days in Chicago at the American Society for Clinical Oncology (ASCO) where I learned about new treatment lines coming out and connecting with other patient advocates.
The cancer research going on now will result in the drugs being used in the coming years. This is why it is so important to preserve funding for the National Institutes of Health. The presidents budget slashes funding by almost 50%. That means many fewer clinical trials and many fewer drugs in 5 years. No one expects to get cancer. If you get cancer in 5 years you will be wishing the NIH had done more research to help you. Please call your elected federal reps and push for restoring funding to NIH.
On a lighter note – Maddy graduated from high school, Evelyn started a research internship at University Colorado Anschutz Medical Campus and we all head to Las Vegas at the end of the month to support Maddy in her last National Dance Competition.
Onward!
Amir humored me with a selfie in front of the MRI machineMaddy’s pre-professional companyThe ASCO meeting was huge with 50,000 attendeesGrateful Nancy could come for the graduationMy 2 favorite future engineers.
Hi everyone. I write this at the end of a long – but good – day. My legs are up in my recliner and the cat is curled up. I guess he had a long day too.
Today was “treatment day.” That means a lab draw, office visit and then infusion of medications.
I had prepared for today and the real possibility of having to change my treatment. As I always say – I want to stay on each line as long as possible because there are a finite number of options.
Short version – I’m staying on my current treatment, Enhertu. I have a very good quality of life with it. It seems to be working, mostly, we think, maybe.
I get this drug every three weeks so I’m estimating that this means I’ll probably stay on Enhertu through a good portion of the summer.
If you are trying to kill time keep reading. Otherwise get outside and grab some sunshine and fresh air! ☀️
Longer version – I’ve been getting PET scans every 3 months for a little over a year. Previous to that I was getting a CT scan with contrast + nuclear bone scan. Recall I had terrible progression and they had to rebuild my upper thoracic spine in November 2023. The CT + bone scans Did. Not. Show. The. Tumors pressing on my spine!
How is this possible? Imaging is a very imperfect science and a lot of it is a matter of interpretation. And why would I get that particular combination of scans? Money. It’s the cheapest option and that is what insurance will pay for, unless something goes terribly wrong.
Queue fall of 2023. We clearly needed better imaging. The insurance company approved a PET-CT scan. PET scans provide essentially the same info as the CT + bone, but honestly they are better. Oncologists prefer them, insurance companies don’t. The PET-CT scan in December 2024 showed more uptake of the tracer in my thoracic spine. Diseased cells take up more of the tracer. These hot spots – or spots of increased uptake could mean the cancer is active and growing (progressing).
I had another PET-CT in March 2025 and it showed even a little more increased uptake in those areas – which made it seem like I was having progression, especially because my (very reliable) blood work tumor markers were steadily rising.
Now, I’ve been at this for a while – almost 6 years actually. I understand what is going on and I know what to ask for. I know that imaging doesn’t really work well for my cancer, unless it’s an MRI. I requested we do an MRI of my thoracic spine to see exactly what was going on. An MRI produces a very detailed image of every part of the internal structure of what is being scanned. My oncologist agreed and I had an MRI last week (on Sunday afternoon no less).
The results of the MRI were – unremarkable! (Love that word!) No tumors growing in my spine. Nothing of note in my thoracic spine. My lumbar spine has some bulging (L1, L2) and severe compression deformities (L3, L4) – which we already knew.
[Side bar – I have lobular breast cancer which typically doesn’t show up well on imaging because it doesn’t clump or form in a lump usually. Also, when it metastasizes it goes to unusual places like the stomach, colon, bowel, bladder and peritoneum and forms in thin sheets or strings, neither of which show up on imaging.]
Image from the Lobular Breast Cancer Alliance showing where mILC can metastasize.
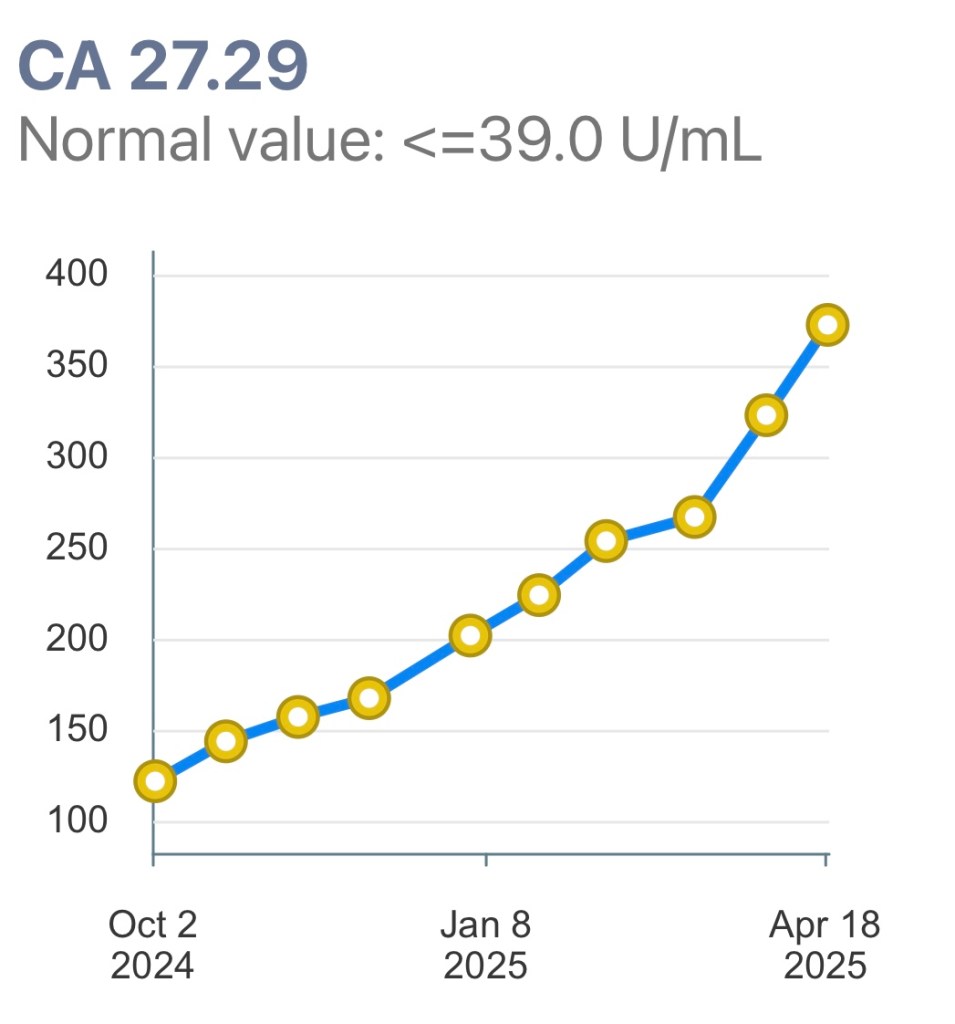
Fast forward to today. My oncologist is totally comfortable with my staying on Enhertu given that the MRI didn’t show anything of concern. My CA 27-29 tumor marker is steadily rising. Historically my tumor marker has been reliable in indicating progression (rising numbers).
Tumor markers give an indication of how active the cancer is. A number below 39 means no active cancer. I’ve never had my tumor marker go below 42 the entire time I’ve had metastatic breast cancer.
My oncologist considers three things when recommending changing medication:
Imaging results
How the patient feels
Tumor markers numbers
Clearly imaging does not do a great job at indicating progression and the MRI didn’t indicate anything alarming. I feel great (working FT, walking an hour a day, just signed up for Pilates 2x a week). My tumor markers suck.
So, stay the course it is. Is this the right decision? 🤷♀️ We think so.
Before I had metastatic cancer, I didn’t appreciate how complicated making decisions was. I’ve learned that science has miles to go improving imaging so that it is more reliable. New in the past few years is the use of measuring circulating tumor cells in the blood, so that may eventually be a tool in the future for oncologists to figure out what is going on and base decisions on.
I appreciate my relationship with my oncologist. Everything is a joint decision. He listens to me (said yes to my suggestion of the MRI). He keeps current on the science and research. We are looking into a possible clinical trial for when it is time to switch medications. I’m grateful that I have access to such good medical care (and currently have very good insurance that allows me such access).
So, my health world right now is good (as are things with the girls). A lot of other parts of life are challenging and stressful. I’ll continue to take things one day at a time and live life to the fullest. I hope you do too. It passes quickly and this is our only chance to seize the day!
Onward!
Today I had a window seat for my infusion. The foothill mountains are green and you can still see snow on the Continental Divide. How wonderful that I have this view.The brown bag has my Enhertu. Once it’s mixed up it can’t be in direct light. I also get fluids (the big bag) and before this I had pre-meds including steroids and 2 kinds of anti-nausea meds. All total I spend ~3 hours at the Cancer Center.